Endotracheal tube insertion depth, to 20 cm in women and 22 cm in men, is more reliable than auscultation for excluding inadvertent endobronchial intubation, especially if the clinician is inexperienced, research shows.
“Tube depth seems to be almost independent of the user’s experience and can be used by clinicians even at the beginning of their training with a high sensitivity and specificity,” Christian Sitzwohl (Medical University of Vienna General Hospital, Austria) and team write in the BMJ.
With auscultation, in contrast, 15% of endobronchial intubations were missed by experienced anesthesiologists, and 55% were missed by first-year anesthesiology residents.
“The hierarchy of the methods used to assess the correct insertion depth should be changed and clinicians should rely more on depth insertion than on auscultation,” say the researchers.
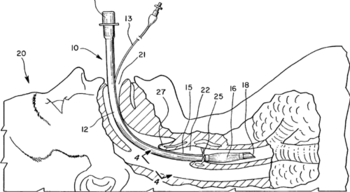
The 164 patients who participated in the study had an endotracheal tube positioned correctly (2.5–4.0 cm above the carina) or incorrectly (in the right mainstem bronchus) by an anesthesiologist using a fibreoptic bronchoscope.
The position of the tube was then independently assessed, using one of three different methods, by an experienced anesthesiologist with at least 2 years of training, and a first-year resident – 32 of the former and 22 of the latter participated in the study.
Overall, auscultation was 65% sensitive and 93% specific for exclusion of endobronchial intubation, whereas tube depth (to 20 cm in women and 22 cm in men) was 88% sensitive and 98% specific. Observation and palpation of symmetrical chest movements was 43% sensitive and 90% specific.
Combining all three techniques had a sensitivity of 100% and a specificity of 95%.
Clinician experience did not significantly influence the chances of a correct diagnosis when tube depth was used as a guide, but being experienced improved the likelihood of a correct diagnosis 10-fold with auscultation and 4.5-fold with observation.
However, the team notes that even experienced clinicians may struggle with auscultation in emergency situations, which often involve patients with underlying respiratory pathology.
Sitzwohl et al observe that the rule of inserting tubes to a depth of 21 cm in women and 23 cm in men (the 21/23 rule) is already in use, but say that following this would have resulted in 20% of women and 18% of men having the tube inserted nearer to the carina than recommended.
Following a 20/22 rule would reduce these rates to 9% and 0%, respectively, they say.